
Definition and Function
The iliac crest is the margin of the ileum. It is a curved, broad structure made to protect the insides of the pelvic region.
It serves as an attachment of muscles, aponeurosis, and fascia of the nearby structures [1].
Iliac Crest Photos of Anatomy: Where is it Located?
The iliac crest is in the middle of anterior and posterior superior iliac spines. The highest part of the iliac crest is at the level of L4 vertebra. The iliac tubercle lies 2 inches behind the anterior superior iliac spine and is at the level of the L5 vertebra [2].

Picture 1 : Surface Anatomy of the Iliac Crest
Image Source: imueos.wordpress.com
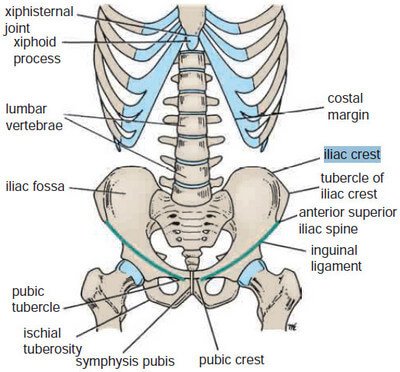
Picture 2: Bones of the Abdomen and Pelvis
Image Source: Snell RS, Clinical Anatomy by Regions 9th edition

Picture 3: The Os Coxae or Costal Bone or Hip Bone
Image Source: endozkop.com
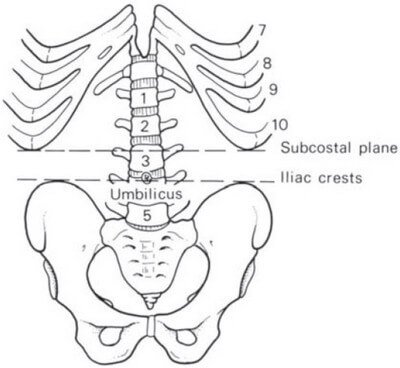
Picture 4: Intercristal Plane at the Level of L4 Vertebra
Image Source: Ellis H, Clinical Anatomy 11th edition
Clinical Importance of the Iliac Crest
Spinal or Lumbar Tap

Picture 5: Bone Marrow Aspiration of the Iliac Crest
Image Source: stemcellthailand.org
The supracristal or intercristal plane which is the highest part of the iliac crest lies at the level of L4 spinous process of the vertebra and in between L4-L5 intervertebral discs. This serves as a landmark in performing the lumbar or spinal tap.
The spinal cord terminates at the level of L1. L4 is a safe area to do the tap in order to obtain cerebrospinal fluid (CSF) sample without damaging the spinal cord.
L4 is also the area where the abdominal aorta bifurcates [1, 2, 3].

Picture 6 : Aortic Bifurcation at L4
Image Source: Ellis H, Clinical Anatomy 11th edition
Iliac Crest Bone Graft
The iliac crest is a common bone that is harvested in bone grafting because of its decompressed form. The iliac crest bone graft is used for spinal fusion.
The source of the bone graft can be autogenous or exogenous.
Autogenous bone graft comes from the patient himself. Although this is considered better than exogenous source because of having the properties capable of osteogenesis, osteoconduction, and osteoinduction, complications are still present. Since it comes from a different body part than the spines, it requires an additional incision to the patient’s body. This increases the risk for infection, bleeding, wound, and pain.
Exogenous bone graft like allograft (from cadavers) only serves as an osteoconductor that allows a bone to form. This option offers the patient to decrease the risk of complications for an autogenous bone graft. However, exogenous bone grafts may be rejected by the receiver’s body since it is not its own [4].
Causes of Pain over the Iliac Crest
Hip Pointer or Iliac Crest Contusion
If a hard hit was forced against the iliac crest, there might be a resulting hematoma of the periosteum of the bone. Swelling and ecchymosis will form over the affected area. Muscles attached to the iliac crest may have spasms. There is pain and immobility over the trunk and hips. The pain is less when the patient walks backwards [5].
If the patient is a runner, training and competition may be contraindicated by sports medicine. However, if the patient can run without limping, he may proceed provided that ice compress and rest will be given to him as soon as possible. Padding with a foam doughtnut pad may be helpful in decreasing mobility of the injured iliac crest [6].
Iliac Apophysitis
Iliac apophysitis is observed among runners too. The patient experiences subtle pain that develops overtime because of chronic irritation to the iliac apophyses. The anterior superior iliac spine was reported to be the most common structure that is being affected.
Physical examination reveals tenderness over the iliac crest. Intensity of pain increases as a practitioner assists the patient in stretching the affected muscle.
To rule out aversion fracture, anteroposterior and oblique radiography should be performed if ossification is noticed. In the absence of ossification, ultrasound may be done.
Iliac apophysitis can be treated with rest, ice, and anti-inflammatory drugs. The pain goes away when the patient has complete abstinence with running for 4-6 weeks [5, 6].

Picture 7 : Causes of Pain over the Iliac Crest
Diagnosis : Iliac Crest Pain

Picture 8: Avulsion Fracture of the Right Iliac Crest
Image Source: rad.usuhs.edu
Anteroposterior and oblique radiography of the pelvis is done in patients who have acute onset of pain to determine the presence of an avulsion fracture [6].
But generally speaking, magnetic resonance imaging (MRI) is not necessary to visualize the underlying tissues because usually, iliac crest pain diminishes overtime, provided that no repeated trauma is introduced into the area [5].
General Treatment for Iliac Crest Pain
- Common sense tells that rest is a must for full and faster recovery.
- Ice application relieves swelling and alleviates inflammation.
- Stretching consoles spasms.
- Range of motion (ROM) exercises are performed to tone and relax the muscles. This allows you to rehabilitate the injured iliac crest.
- Electrical stimulation minimizes the pain.
- Anti-inflammatory drugs alleviates the pain.
- Use of crutches limits mobility of the affected area, thereby preventing further pain episodes [5].
References:
- Moore KL et al, Clinically Oriented Anatomy 6th edition, Lippincott Williams & Wilkins 2010, p 514
- Snell RS, Clinical Anatomy by Regions 9th edition, Lippincott Williams & Wilkins 2012, p 151
- Ellis H, Clinical Anatomy 11th edition, Blackwell Publishing 2006, p 55
- Galler RM & Sonntag VKH, Bone Graft Harvest, Barrow Quarterly Vol 19 No 4, 2003 accessed on http://www.thebarrow.org/Education_And_Resources/Barrow_Quarterly/205303
- Starkey C, Athletic Training and Sports Medicine: An Integrated Approach, Jones & Bartlett Publishers 2011, pp 234-236
- McMillan JA et al, Oski’s Pediatrics: Principles & Practice, Lippincott Williams & Wilkins 2006, p 893

