
Definition and Function
Lingual tonsils are a group of lymphoid nodules (30-100 follicles) located at the posterior third of the tongue.
Their appearance is described as exophytic mucosal small masses with crypts and folds. This creates the reticular pattern at the base of the tongue. Its precise location is between the circumvallate papillae and the lining of vallecula that extends to the root of epiglottis [1, 2].
The tonsils are parts of the lymphatic system that wards off harmful substances and infection. The lingual tonsil basically protects us from upper respiratory tract infections.
The lingual tonsil enlarges from birth until the person reaches 7 years of age and eventually shrinks as one grows old [3].
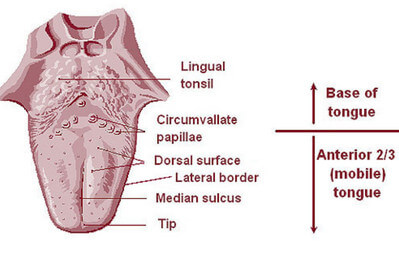
Picture 1: The Dorsum of the Tongue
Image Source: en.wikipedia.org

Picture 2: Sagittal Section of the Oral Cavity
Image Source: studyblue.com

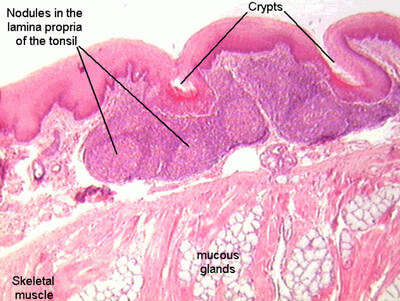
Picture 3: Lingual Tonsil Histology
Image Source: cea1.com
Picture 4: Lingual Tonsil Histology
Image Source: php.med.unsw.edu.au
The lingual tonsil is lined by a nonkeratinizing squamous epithelium. A definitive histological feature of a tonsil is the presence of tonsillar crypts. These start to appear after birth. Lingual tonsils have shallower crypts and appear less branched when compared to palatine tonsils.
Other important structures observed under the microscope are the lymphoid follicles, mucous salivary glands, skeletal muscles, and adipose tissue.
The lymphatic vessels of the posterior portion of the tongue pass through the pharyngeal wall around the external carotid artery and drain into the deep cervical lymph nodes [4].
Clinical Correlation
Enlarged and Swollen Lingual Tonsil
The lingual tonsil becomes enlarged and painful in the presence of inflammation, allergy, or infection. It can also happen as a compensatory mechanism after the patient has undergone tonsillectomy or adenoidectomy.
Normally, the lingual tonsils have a reticular pattern on its surface. With hypertrophy of the lingual tonsils, this pattern will be disturbed.
Frontal view of the radiograph will show 5-7 mm, smooth surfaced nodules in patients with lymphoid hyperplasia. Laterally, these nodules distend posteriorly. In severe cases, these nodules reach the vallecula.
Unilateral enlargement of the lingual tonsil warrants tissue biopsy in order to rule out lymphoma or squamous cell carcinoma [1, 2]. Lymphoma increases in size and is more likely to obstruct the airway. Squamous cell carcinoma, on the other hand, is the more common type of cancer of the lingual tonsil. It appears as ulcers at the back of the throat [5].

Picture 6: Lingual Tonsil Obstructing the Airway
Image Source: Kummer A, Cleft Palate & Craniofacial Anomalies: Effects on Speech and Resonance, Cengage Learning, 2007
The lingual tonsil is located at the back of the tongue, meaning it is close to the airway. With its enlargement, it may cause airway obstruction and breathing difficulties. It may come to a point where the larynx cannot be seen and the vallecula may be covered with tissues of the lingual tonsil, as illustrated above [6].
Lingual Tonsillitis
Picture : Lingual Tonsillitis
Image Source: simple-health-secrets.com
Lingual tonsillitis is primarily presented as a complaint of pain over the hyoid bone, which may be unilateral or bilateral. Upon physical examination, the lingual tonsils appear swollen and exudates are noted to be present. Other signs and symptoms include fever, dysphagia (difficulty in swallowing), tenderness over the affected area, lymphadenopathy, and muffled voice [7].
More often than not, bacteria is the cause of lingual tonsillitis so preliminary antibiotics is being prescribed. Throat swab is obtained and cultured. If bacteria is ruled out to be the cause, antibiotics will be discontinued. If lingual tonsillitis is caused by a virus, symptomatic treatment will be ensued. Pain medications will be prescribed. Gargling with saline solution seems to work well [5].
Picture : Oral Lymphoepithelial Cyst or Cystic Ectopic Lymphoid Tissue
Image Source: intechopen.com
The most common locations of oral lymphoepithelial cysts or cystic ectopic lymphoid tissue are the lateral sides of lingual tonsils, floor of the mouth, and tongue surface.
This occurs when the tonsillar crypts become housed with keratin and this will form the cysts. They appear as whitish or reddish yellow dome-shaped nodules. These cysts will enlarge due to inflammatory or allergic reactions. Airway obstruction warrants its removal [8].
Lingual Tonsillectomy
Indications for lingual tonsillectomy include its enlargement causing airway obstruction and obstructive sleep apnea, chronic and recurrent infections, and cancer or malignancy.
Under general anesthesia, the tongue is pulled out with the lingual tonsils clamped. Preferred removal of the lingual tonsil is through laser or cautery in order to minimize bleeding.
Watch out for postoperative hemorrhage. Aspirin is contraindicated post-tonsillectomy to avoid bleeding.
Postoperative pain is most intense for the first two days then it wanes off. Four to six days after surgery, the pain comes back and this time, the pain radiates to the ears. Scabs will develop at the back of the throat and this may cause halitosis (bad breath).
After the surgery, pain medications are prescribed in order to relieve the discomfort. Antibiotics are given for halitosis and to prevent postoperative infection. These will be taken in for 10 days. Ice chips or popsicles may help ease the swelling.
Typically, the post-operative patient may resume clear fluid diet followed by soft diet then diet as tolerated. The patient should not eat hot, spicy, acidic, sour, rough, and scratchy foods because these will add up to the already agonizing pain.
If the lingual tonsil is verified as cancerous or malignant, chemotherapy, radiation therapy, and another surgery may be necessary [9].
References:
- Ekberg O & Aksglaede K, Radiology of the Pharynx and the Esophagus, Springer Science & Business Media, 2004, pp 60-61
- Bruch JM & Treister N, Clinical Oral Medicine and Pathology, Springer Science & Business Media, 2009, pp 5 & 19
- http://www.innerbody.com/anatomy/nervous/lingual-tonsil-side#full-description
- Cardesa A & Slootweg P, Pathology of the Head and Neck, Springer Science & Business Media, 2006, p 184
- http://www.wisegeek.org/what-is-a-lingual-tonsil.htm
- Kummer A, Cleft Palate & Craniofacial Anomalies: Effects on Speech and Resonance, Cengage Learning, 2007, p 288
- Interpreting Signs & Symptoms, Lippincott Williams & Wilkins, 2008, p 591
- Burket LW, Burket’s Oral Medicine, PMPH-USA, 2003, p 114
- http://advancedotolaryngology.com/patient-education/tonsillectomy/